Your Results
Understanding your results
Your test produces a curve. Here’s what it means.
What your curve tells you
This is what makes the Heidelberg test unique. Your stomach is challenged, and the curve shows exactly how it responds. Eight distinct patterns. Each one tells a different story.
Pattern 1
Normal Reacidification
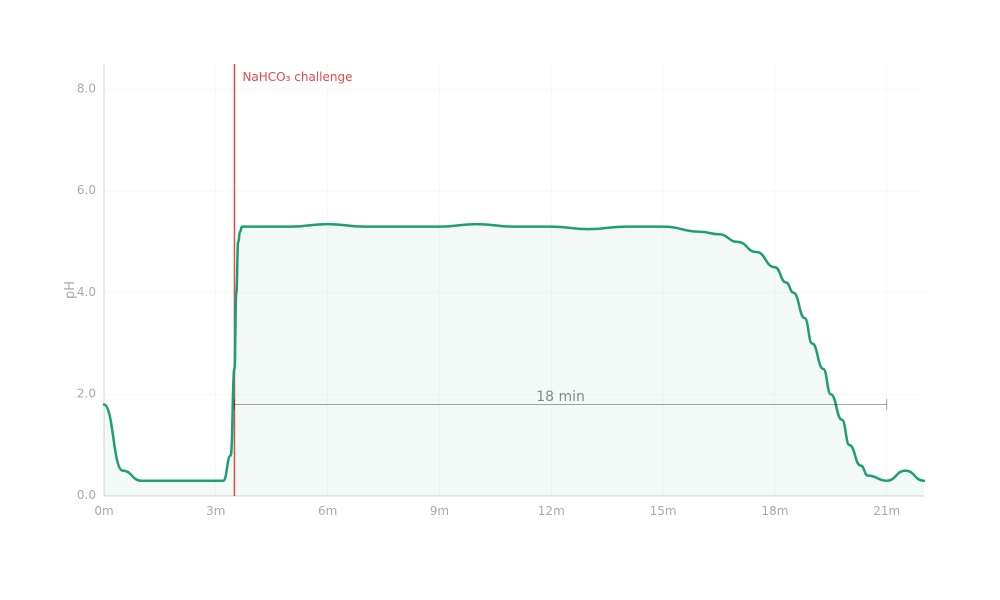
Before the challenge, your stomach acid is sitting exactly where it should be. Strong and low.
When the bicarbonate solution hits, the pH jumps up. That's expected. The alkaline solution temporarily neutralizes your acid. For about 15 minutes, your stomach fights back. It's producing acid the whole time, but the bicarbonate is holding its ground. The two forces are in a tug of war.
Then around the 18-minute mark, your stomach wins. The acid overwhelms the bicarbonate and the pH drops back down fast. Not a slow fade. A decisive drop.
This is what healthy looks like. Your parietal cells are working, your acid production is strong, and your stomach can fully recover from a challenge within a normal timeframe.
Pattern 2

Hyperchlorhydria
Your stomach is producing too much acid. Way too much.
When the capsule first lands, the pH drops fast to a strongly acidic level. That tells us the resting acid environment is already intense.
Then the challenges begin. Four rounds of bicarbonate, one after another. Each time, your stomach overwhelms the solution in under 10 minutes. There is no plateau, no sustained tug of war. The acid overcomes the bicarbonate and the pH drops right back down. Every single time.
That kind of response means your parietal cells are not just working, they are overproducing. The stomach is not slowing down between rounds. It is sustaining maximum output without fatigue.
This pattern is hyperchlorhydria. Too much acid, too fast, too consistently. Understanding this gives you and your practitioner a clear starting point for deciding what to do next.
Pattern 3
Extreme Hyperchlorhydria
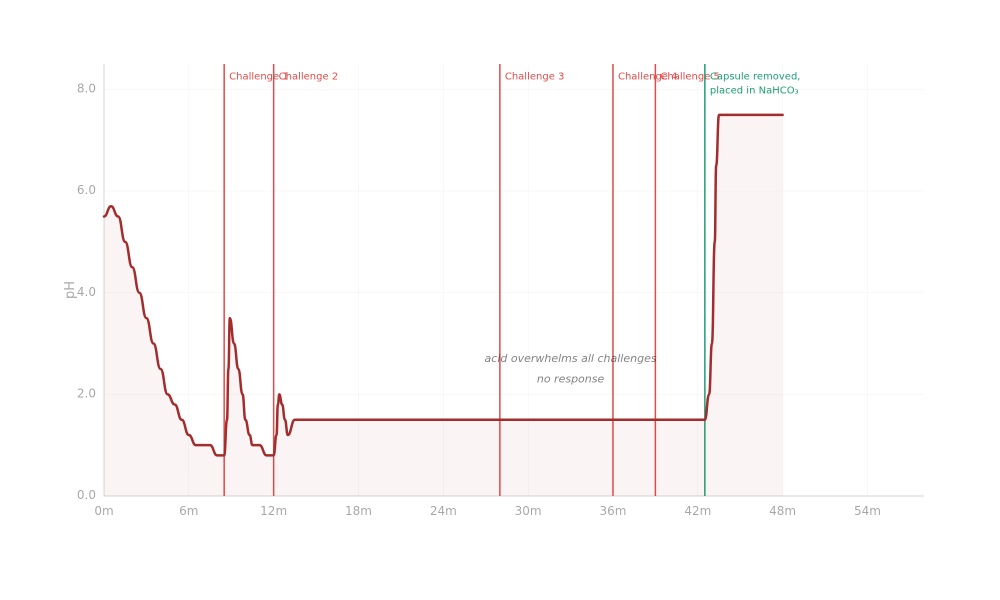
This is acid production at its most intense. The stomach is strongly acidic at rest, and when the first challenge hits, it barely makes a dent. The pH rises slightly, then drops right back down almost immediately. Not in ten minutes. In seconds. The second challenge has even less impact.
Then something remarkable happens. Challenges 3, 4, and 5 go in, and the curve does not move at all. The pH stays flat. The stomach is neutralizing the bicarbonate the instant it arrives. The solution never even gets a chance to register on the curve.
At the end of the test, the practitioner retrieves the capsule and places it directly into a bicarbonate solution outside the body. The pH jumps immediately, confirming the sensor was working perfectly the whole time. That flat line was not a malfunction. It was the stomach producing acid so aggressively that the standard challenge could not keep up.
This is rare, and it is significant. This level of acid output warrants further investigation with your practitioner to understand what is driving it.
Pattern 4

Hypochlorhydria
At first, everything looks normal. The resting acid level is right where it should be. Then the challenge goes in, and the pH jumps up. So far, so expected.
Then nothing happens. For 42 minutes.
The pH just sits there. Flat. The stomach is trying to make acid, but it can't produce enough to overcome the bicarbonate. In a healthy stomach, this fight is over in under 20 minutes. Here, the buffer is winning for more than twice as long.
Eventually the stomach does recover. The pH drops back down, and when it does, it drops fast. So the acid-producing cells aren't dead. They're working. They just can't keep up.
This is hypochlorhydria. The stomach can make acid, just not enough. It's the most common finding on Heidelberg testing, often seen in people over 50, people who have been on PPIs long term, and people with early changes to their stomach lining.
This is exactly the kind of information that helps you and your practitioner understand what's actually going on, rather than guessing.
Pattern 5
.jpg)
Fatiguing Hypochlorhydria
The resting acid looks fine. The stomach is producing acid at baseline. Then the challenge goes in, and the pH shoots up. Normal so far.
But what happens next is different from anything else. There's no plateau. There's no decisive drop. Instead, the pH comes down slowly, unevenly, over the course of nearly an hour.
The stomach is fighting, but it's struggling. The acid output surges, then fades, then surges again. The curve is jagged and inconsistent. It's like watching someone try to push a boulder uphill and keep losing their grip.
It takes 58 minutes to get back to baseline. A healthy stomach does this in under 20.
The acid-producing cells aren't gone. They're there, they're trying. But they're running out of steam. They can't sustain the output needed to overcome even a single standard challenge in a normal timeframe.
This pattern is often seen in people with long-term PPI use, progressive changes to the stomach lining, or chronic inflammation. It tells a very specific story: your stomach can still make acid, but it's working at the edge of its capacity. That's the kind of clarity that changes how you and your practitioner approach what comes next.
Pattern 6

Achlorhydria
Something unusual is clear from the moment the capsule lands. There is no acidic baseline. The pH sits around 6.5, essentially the same as the mouth. It does not change. There is no acid production. This is achlorhydria.
In a normal test, the baseline would be strongly acidic and a bicarbonate challenge would follow. Here, there is nothing to challenge. The stomach is already alkaline. So the practitioner shifts to a different approach.
You are given betaine HCl capsules. This is supplemental acid, delivered directly into the stomach to see whether the environment can even become acidic at all. The pH starts to drop slowly. More capsules go in. Eventually the stomach reaches a strongly acidic level. But none of that acid came from your body. All of it came from the capsules.
Then the most revealing part. Once the betaine wears off, the pH climbs right back up. Over the next 30 minutes, the stomach drifts back toward alkaline. It cannot hold onto the acidity it was given. There is zero acid production of its own to sustain it.
This is the most significant finding on Heidelberg testing. Complete absence of stomach acid production. This pattern may indicate that protein digestion, nutrient absorption, and the stomach's natural barrier against bacterial overgrowth are affected. It gives you and your practitioner a clear, measurable understanding of what is happening so you can determine the right steps forward together.
Pattern 7
Hidden Hypochlorhydria
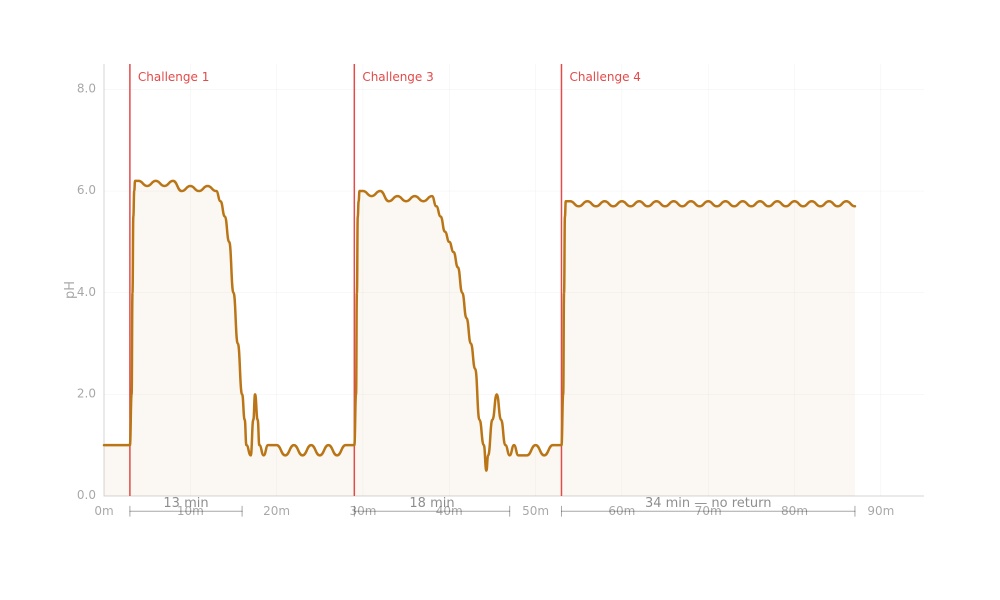
At first glance, this stomach looks normal. The resting acid is strong, sitting right where it should be. The first challenge goes in, the pH rises, and the stomach fights back. It recovers in 13 minutes. A bit slower than the fastest pattern, but still within a normal range. If the test stopped here, you would think everything was fine.
It is not.
Challenge two goes in. The stomach recovers again, but this time it takes 18 minutes. Five minutes slower. The acid-producing cells are starting to tire.
Challenge three is where it gets real. The pH rises, and the stomach tries to respond. But this time it cannot finish the job. After 34 minutes, the pH is still elevated, gently drifting. The stomach has stopped fighting. The cells that responded to the first challenge have nothing left to give.
This is the pattern that hides in plain sight. A single challenge would have looked normal. But the stomach is a sprinter, not a marathon runner. It can produce acid in short bursts, but it cannot sustain output under repeated demand. Only a multi-challenge test exposes this, and that is exactly what the Heidelberg test is designed to do.
Pattern 8
Bile Reflux
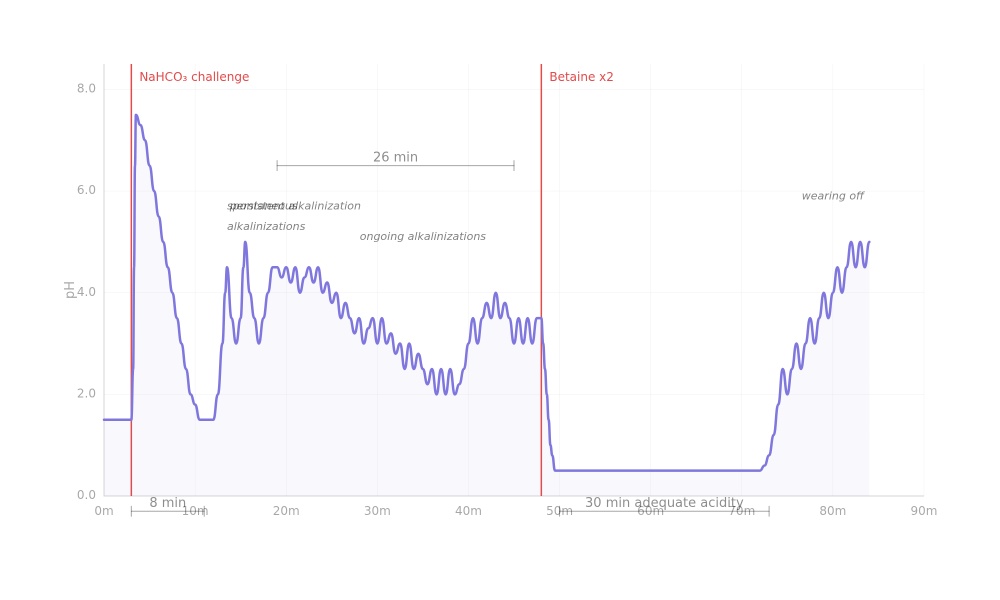
The first part of this test looks completely normal. The resting acid is strong, the challenge goes in, and the stomach recovers in 8 minutes. If the test ended here, you'd walk away thinking everything was fine.
But the test continues. And the story changes completely.
After recovery, the pH starts behaving erratically. It jumps up, drops down, jumps again. Sharp alkaline spikes keep interrupting what should be a stable acidic baseline. This goes on for 26 minutes. No bicarbonate is being given. These spikes are coming from inside your body.
What's happening is bile. Alkaline contents from the small intestine are washing back up through the pyloric valve into the stomach. Each spike on the curve is a wave of bile disrupting the acid environment. The stomach tries to recover after each one, but before it can stabilize, another wave hits. The result is a chaotic, oscillating pattern that looks nothing like any of the acid insufficiency patterns.
To confirm, your practitioner gives you betaine HCl to flood the stomach with acid. The pH drops and holds steady. This proves the acid-producing cells are working perfectly. The problem isn't acid production. It's the valve. Bile is getting in where it shouldn't be.
This matters because bile reflux can look like low stomach acid on a superficial test. The pH is elevated, so it's easy to assume the stomach isn't making enough acid. But that conclusion would be wrong, and the approach would be completely different. A real-time pH curve gives your practitioner the data to understand what's actually driving the pattern, and that changes everything about the approach.
Unlock the truth of your stomach acidity.
See if the Heidelberg test is your next step.